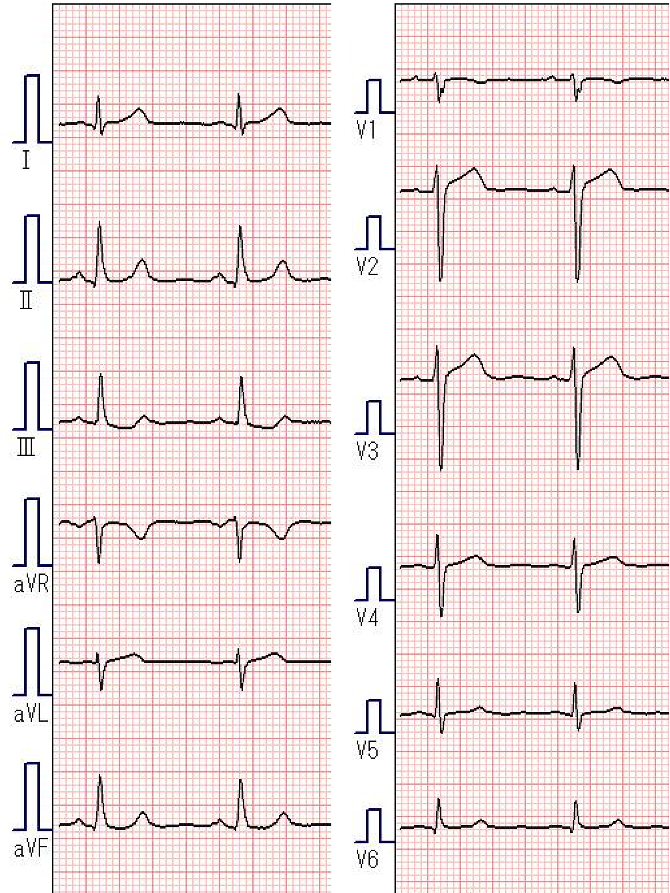
ECG
Blood Test
Liver function: Normal
Renal function: Normal
TC 183mg/dL
HDL 50mg/dL
LDL 96mg/dL
TG 184mg/dL
FBS 113mg/dL
HbA1c 5.4%
NTproBNP 40pg/mL
UCG (before PCI)
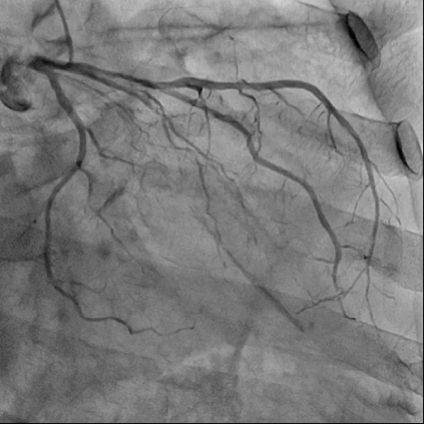
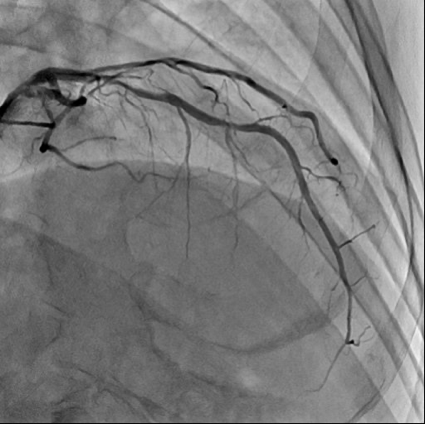
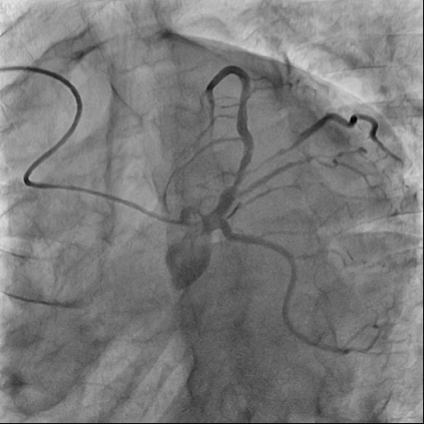
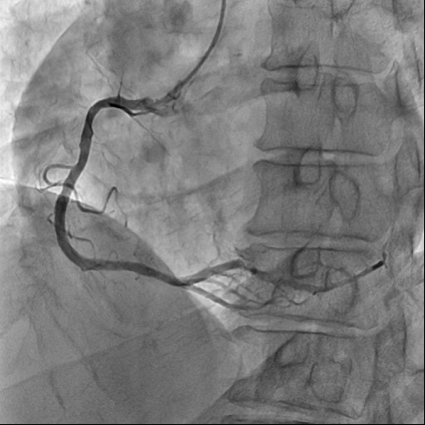
CAG
PCI
Pre angio
Pre angio
Post LAD/D1 T stenting
Post LM stenting
IVUS
PCI(Final angio)
Two weeks after outpatient examination
Potentially diastolic murmur?
UCG (2 months after PCI)
TEE (4 months after PCI)
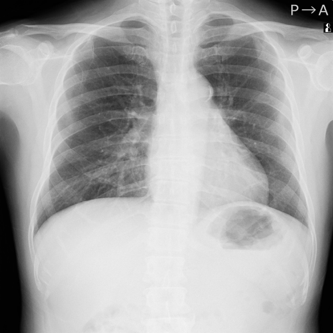
BXP
Before PCI
6 months after PCI
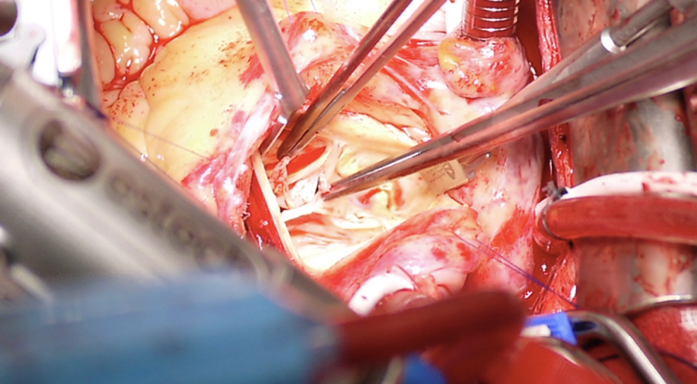
Aortic valve under direct observation
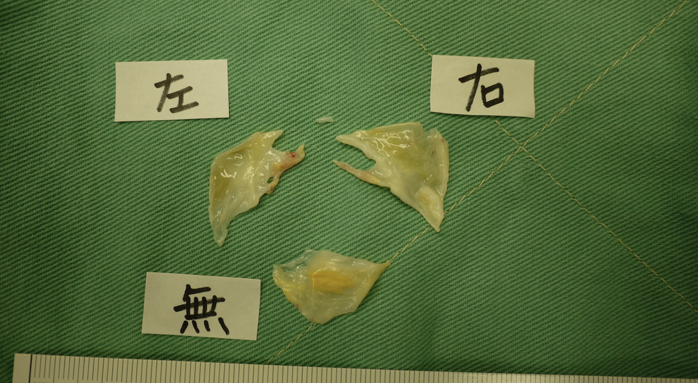
Valvular fragments
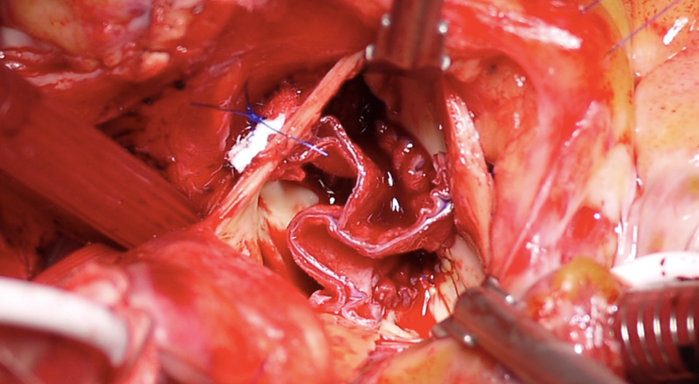
Aortic valvuloplasty(The Ozaki Method)
Summary
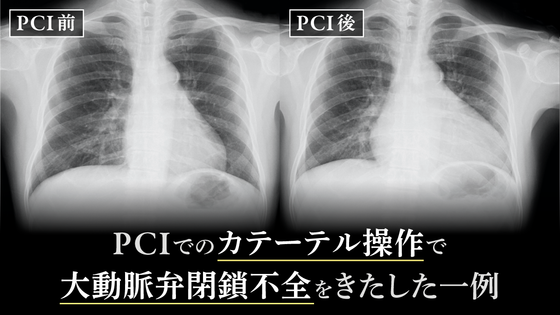
Aortic regurgitation occurred during PCI of a left main lesion.
The immediate post-PCI course was good, but after six months, the patient developed symptomatic heart failure.
Aortic valvuloplasty was performed 10 months after PCI.
Discussion
First of all, the left coronary artery was quite posterior and started from a slightly elevated position. An extra catheter was used, which was difficult to engage during the procedure causing the guiding catheter tip to push against the aorta which possibly resulted in damaging the valve. As the other possible cause of the valvular damage, the patient was thought to have some kind of congenital anomaly in his body due to his short stature and gait disorder. The surgeon in charge of the operation commented that the valve was much weaker than usual. This case reminded us of the importance of daily auscultation in the outpatient clinic, because guiding catheter operations may cause aortic injury or aortic valve injury.
Comment from Dr. Kimura
Because of the young age of the patient, we performed an autologous pericardial valve replacement (AVNeo) without anticoagulation. The patient is now doing well after the surgery.
Dr. Osamu Matsuda
2002
Graduated from Hiroshima University
2002
Internship in Internal Medicine, Hiroshima University
2004
Department of Cardiology, Hiroshima City Asa Citizens Hospital
2007
Department of Cardiology, JA Onomichi General Hospital
2008
Toyohashi Heart Center
2008
Nagoya Heart Center
2015
Hiroshima Heart Center
Dr. Hiroyuki Kimura
1995
Graduated from Kurume University School of Medicine
1995
Department of Internal Medicine, Hiroshima University Hospital
1996
Department of Cardiovascular Medicine, Hiroshima Prefectural Hospital
1997
Department of Cardiology, Hiroshima City Asa Citizens Hospital
2000
First Department of Internal Medicine, Hiroshima University Hospital
2004
Graduate School of Medicine, Hiroshima University
2004
Department of Cardiology, Lenox Hill Hospital, USA
2005
Columbia University Medical Center, USA
2007
Toyohashi Heart Center
2014
Japan Senoo Cardiology and Cardiovascular Surgery
2016
Hiroshima Heart Center